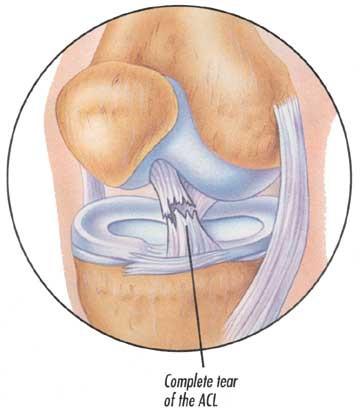
The anterior cruciate ligament is one of the major stabilizing ligaments in the knee. It is a strong rope like structure located in the center of the knee running from the femur to the tibia.
When this ligament tears it lacks the ability to heal and can lead to the feeling of instability in the knee.
ACL reconstruction is a commonly performed surgical procedure and with recent advances in arthroscopic surgery can now be performed with minimal incisions and low complication rates.
The ACL is the major stabilizing ligaments in the knee. It prevents the tibia (Shin bone) moving abnormally on the femur (thigh bone). When this abnormal movement occurs it is referred to as instability and the patient is aware this abnormal movement.
Often other structures such as the meniscus, the articular cartilage (lining the joint) or other ligaments can also be damaged at the same time as a cruciate injury & these may need to be addressed at the time of surgery.
Once the initial injury settles down the main symptom is instability or giving away of the knee. This usually occurs with running activities but can occur on simple walking or other activities of daily living.
The diagnoses can often be made on the history and physical exam alone. The physical exam reveals the instability caused by an ACL tear.
An MRI can be helpful if there is doubt or to provide additional insight as to other injuries to the knee
Not everyone needs surgery. Some people can compensate for the injured ligament with strengthening exercises or a brace. However, most patients opt for surgery as bracing and exercise can only particularly compensate for the instability after ACL injury. Patients with an ACL tear are at additional risk to damage other structures about the knee and for development of arthritis
Young patients wishing to maintain an active lifestyle.
Sports involving twisting activities e.g., Soccer, netball, football Giving way with activities of daily living.
People with dangerous occupations e.g., Policemen, firemen, roofers, scaffoulders.
It is advisable to have physiotherapy prior to surgery to regain motion and strengthen the muscles as much as possible.
Surgical techniques have improved significantly over the last decade, complications are reduced and recovery much quicker than in the past.
The surgery is performed arthroscopically. The ruptured ligament is removed and then tunnels (holes) in the bone are drilled to accept the new graft. This graft which replaces your old ACL is taken either from the hamstring tendon or from an allograft (tissue bank tendon). There are advantages & disadvantages of each with the final decision based on surgeon’s and patient’s preference.
The graft is prepared to take the form of a new tendon and passed through the drill holes in the bone.
The new tendon is then fixed into the bone with various devices to hold it into place while the ligament heals into the bone
Other injuries to the knee can be clearly visualized at the same time and any other damage is dealt with e.g., meniscal tears.
Surgery is performed as an outpatient.
Typically patients can fully weight bear within a few days. Physical therapy can be started a few days after surgery to regain strength and function in the injured knee
Physiotherapy is an integral part of the treatment and is recommended to start as early as possible. Preoperative physiotherapy is helpful to better prepare the knee for surgery. The early aim is to regain range of motion, reduce swelling and achieve full weight bearing.
The remaining rehabilitation will be supervised by a physiotherapist and will involve activities such as exercise bike riding, swimming, proprioceptive exercises and muscle strengthening. Cycling can begin at 3-4 weeks and jogging can generally begin at around 2-3 months. The graft is generally strong enough to allow return to all sports at around 6 months.
The rehabilitation and overall success of the procedure can be affected by associated injuries to the knee such as damage to meniscus, articular cartilage or other ligaments.
The following is a more detailed rehabilitation protocol useful for patients and physiotherapists. It is a guide only and must be adjusted on an individual basis taking into account pain, other pathology, work and other social factors.
With respect to hamstring loading, they should never be pushed into pain and should be carefully progressed. Any subtle strain or tightness following exercises should be managed with a reduction in hamstring based exercises
Prior to running certain criteria must be met
A safe return to sporting activities
Treatment Guidelines
Complications are not common but can occur. Prior to making the decision of have this operation. It is important you understand these so you can make an informed decision on the advantages and disadvantages of surgery.
These can be Medical (Anaesthetic) complications and surgical complications
Medical complications include those of the anaesthetic and your general well being. Almost any medical condition can occur so this list is not complete. Complications include
Allergic reactions to medications. Complications from nerve blocks such as infection or nerve damage.. The following is a list of surgical complications. These are all rare but can occur. Most are treatable and do not lead to long term problems.
Approximately 1 in 200. Treatment involves either oral or antibiotics through the drip, or rarely further surgery to wash the infection out.
These are clots in the veins of the leg. If they occur you may need blood thinning medication in the form of injections or tablets. Very rarely they can travel to the lung (Pulmonary Embolus) which can cause breathing difficulties or even death.
This is due to bleeding in the soft tissues and will settle with time.
Can result from scar tissue within the joint, and is minimized by advances in surgical technique and rapid rehabilitation. Full range of movements cannot always be guaranteed.
The graft can fail the same as a normal cruciate ligament does. Failure rate is approximately 1-2%. If the graft stretches or ruptures it can still be revised
These are small nerves under the skin which cannot be avoided and cutting then leads to areas of numbness in the leg. This normally reduces in size over time and does not cause any functional problems with the knee. Very rarely there can be damage to more important nerves or vessels causing weakness in the leg.
All grafts need to be fixed to the bone using various devices (hardware) such as screws. Rarely, the screws can loosen or break
Donor site means where the graft is taken from. In general the hamstrings tendons are used. These can be pain or swelling in these areas which usually resolves over time.
Can occur especially if there is damage to other structures inside the knee.
An extremely rare condition that is not entirely understood, which can cause unexplained and excessive pain.
Anterior Cruciate Ligament reconstruction is a common and very successful procedure. In the hands of an experienced surgeon, 95% of people have a successful result. It is generally recommended in the patient wishing to return to an active lifestyle especially those wishing to play sports involving running and twisting.
 Menu
Menu